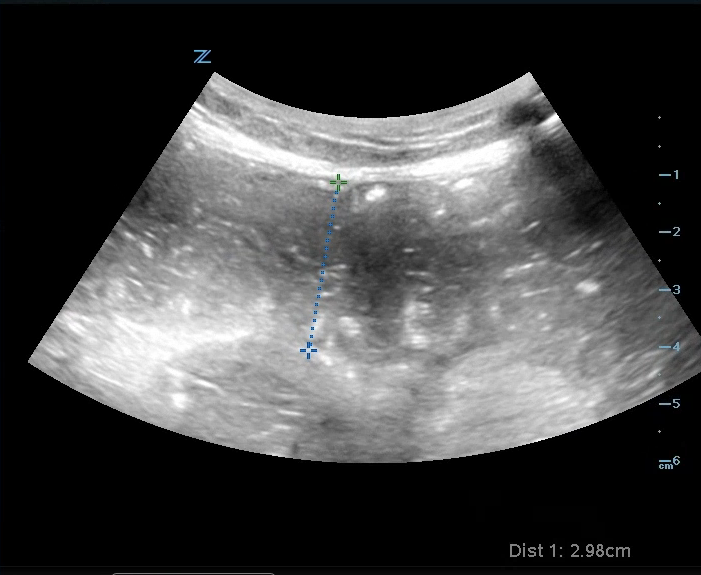
Case: 57 yoF with PMHx of osteoarthritis presented to the ED with right knee pain. A bedside US was performed that showed bulging of the right medial meniscus with surrounding edema Image 1, videos 1&2), consistent with a tear in the medial meniscus.


Meniscal Tear
How to assess the meniscus:
Have the patient flex their knee slightly to 20-30 degrees (you can prop their knee up with a rolled towel)
Use the linear probe and place it longitudinally along the medial aspect of the knee
Identify the medial collateral ligament (MCL), which will appear as a hyperechoic and fibrillar structure, extending from the medial femoral condyle to the proximal tibia
The meniscus will appear as a triangular structure that sits between the femur and tibia, under the MCL

5. A meniscal tear is identified with a well-defined anechoic or hypoechoic area surrounding the meniscus. It can cause extrusion of the meniscus as a result of surrounding edema, described as a "muffin top". There may also be increased vascularity in the surrounding area when color flow doppler is applied
Note: The same process can be repeated on the lateral aspect of the knee to assess the lateral meniscus (image 3).

Case conclusion: While the patient had pain with flexion, she was able to ambulate independently. She was discharged with orthopedic follow-up and conservative measures.
Happy scanning!
Ariella Cohen
References:
https://theultrasoundsite.co.uk/ultrasound-case-studies/
https://ultrasoundpaedia.com/knee-normal/
https://www.nysora.com/ultrasound-of-the-musculoskeletal-system/chapter14-knee-preview/