You get a notification: GIB. Hypotensive.
Patient arrives and they’re vomiting blood with a soft BP.
Do you send for emergent blood? Do you initiate MTP? Do you crack the fridge? What does “crack the fridge” mean? :O
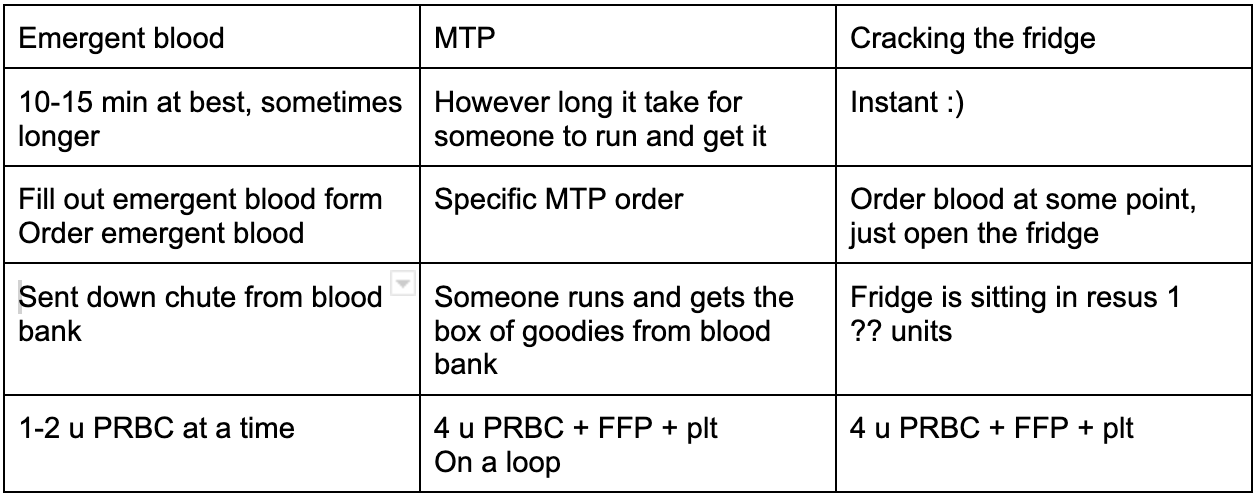
A chart comparing MTP, emergency blood transfusion, and “cracking the fridge” are attached, for a general overview.
Type O blood for all 3.
O positive for men b/c they don’t have Rh factor so it doesn’t matter for them
O negative for women just in case they are Rh negative
Emergent blood
Patient can’t wait for cross-matched blood but they’re not SOO unstable that you need to crack the fridge. Could wait 10-15 minutes.
Print “emergency blood transfusion request” form from Taylor health (shown below)
Can do 1 or 2 units at a time. If you’re NOT running both bags at the SAME time, please order just 1 unit at a time.
“Crack the fridge”
Cracking the fridge does NOT automatically initiate MTP but because it often goes with it, PLEASE clarify with your team whether you are initiating MTP or not when you crack the fridge.
Fridge contents: 4 u PRBC, 4 FFP, 1 platelets = 1st round of MTP
The code is your attending’s 4 digit callback number, or the nurses have a number.
To replace the fridge contents, just call the blood bank to restock.
Pictured below: the blood fridge. Code entered via touchscreen.
Contents of the fridge also shown
Massive Transfusion Protocol, or MTP
Patient needs ALL THE BLOOD.
Often used hand in hand with the fridge blood because they need it all and they need it fast
MTP: The process.
Same taylor health form as emergency blood, shown above
“The box” - 4 PRBC, 4 FFP, 1 platelets in the first round
Ror round two and onwards, same as round 1 but with cryoprecipitate if requested for very very bleedy patients
Usually you crack the fridge, start using the 2 units in the fridge and call up to blood bank and they will continue to prepare more units
When MTP is activated, resources are diverted to preparing blood for the ED.
Primarily ties up the techs to prepare MTP. So places like the OR can’t get blood b/c all the blood bank techs are pulled to prepare more products for the MTP, until the MTP is done.
Use wisely but obviously use it when you need to
MUST send someone from ED up to blood bank to get it, since the products are supposed to be in a cooler
This is the rate limiting step in getting the first box from blood bank, but this is why you crack the fridge first, to initiate MTP while waiting on blood bank
MTP: why do it?
Patients with severe hemorrhage might actually get refractory hemorrhage due to:
Dilution of clotting factors (plts, fibrinogen)
Hypothermia from transfusion of cold products
Hypocalcemia induced coagulopathy
Acidosis
MTP allows for balanced transfusion including clotting factors
When should you do MTP?
NO set criteria for it. Based on clinical judgement.
Hemoglobin level has LITTLE benefit in determining need for MTP
Hypotension also is usually a late manifestation of hemorrhage so don’t always go solely off BP
Coagulation labs?
You can’t actually trend these reliably b/c blood products are given so rapidly
Thus, blood products are administered empirically in a 1:1:1 ratio of PRBC:FFP: Plt
What about cryoprecipitate?
Fibrinogen may become depleted in massive transfusion due to dilution and there might not be enough fibrinogen in FFP
In the US, cryoprecipitate is commonly used for fibrinogen supplementation.
10 u cryoprecipitate should increase fibrinogen by ~75 mg/dL
Target fibrinogen > 150-200 mg/dL
Diff hospitals have diff protocols for fibrinogen supplementation. Ours is described above.