Today we are going to try to focus on a practical skill which is increasingly important with our aging population: Fragile Skin Tears. Hemostasis/Pain Control:
Pressure
Use LET (Lidocaine-Epinephrine-Tetracaine)!
Topical TXA
Surgicel
Suture Techniques:


Apply a couple deep sutures to appose the wound edges. Then place steri strips across the wound and suture through them with 4.0 nylon sutures. This places tension on the tissue below rather than just on the skin.
Place steri-strips parallel to the wound and suture through the steri strips with 4.0 nylon suture. Similar to approach above, however you are able to visualize the wound edges.
Derma-Bond AND Steri Strips. Perform the above techniques, however derma-bond the edges of the wound, let dry, and place sutures through both the steri strips and derma bond. This will be the effective technique for preventing shearing of extremely fragile skin.
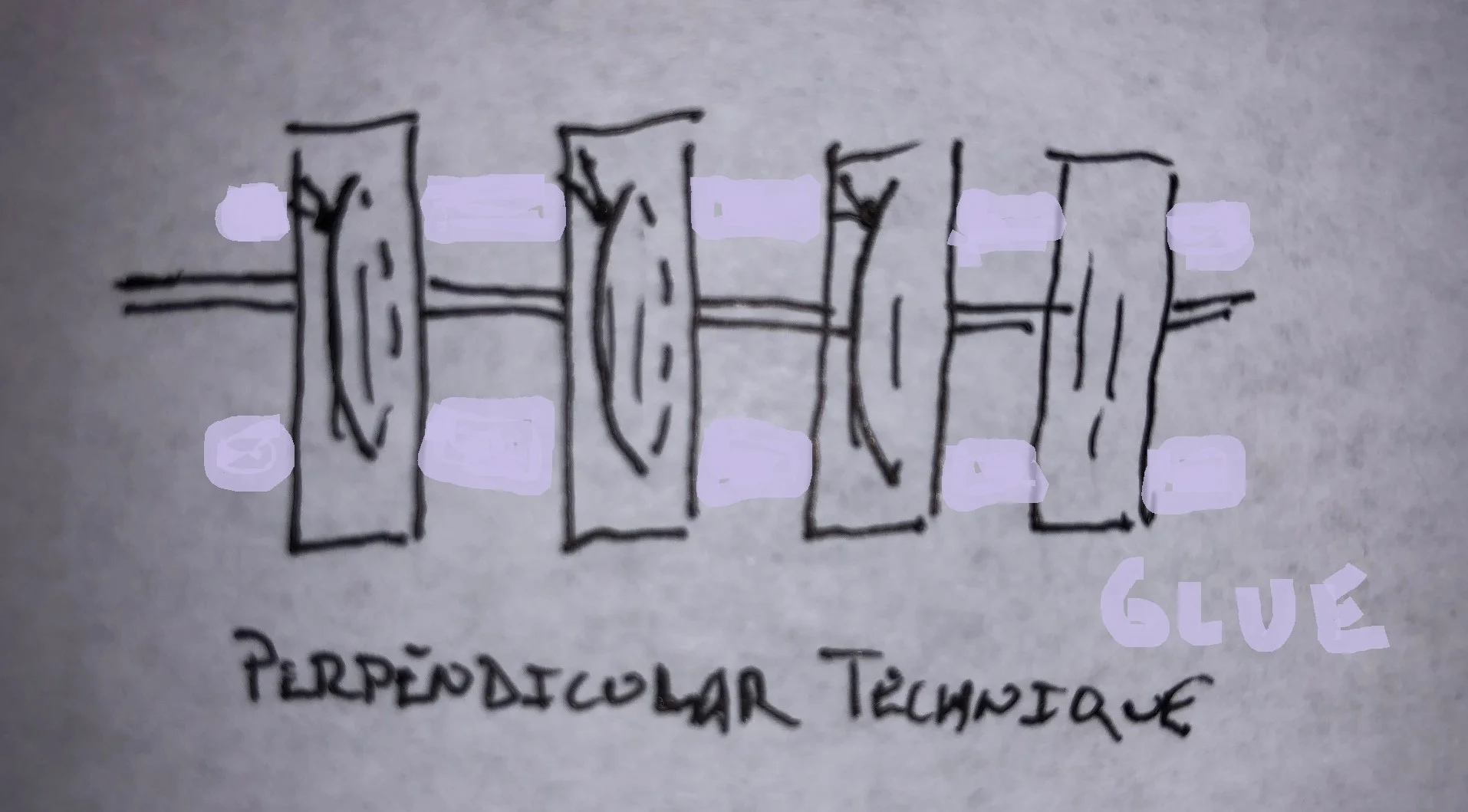
Note there are many variations to this, you may also throw sutures behind the glue. Glue alone may work better for jagged edges than steri-strips.
Mattress sutures, tegaderm and wait etc.
Aftercare
When the steri strip techniques are used, try to keep wound dry (rather than using topical antibiotics such as bacitracin which will cause the steri strips to become ineffective. Patients should be vigilant for signs of infection.
Sources:
EMDocs
Lacerationrepair.com
Aliem
Search Terms: Elderly Skin Parchment Laceration Fragile Skin Laceration Tear