Did you know that over the holidays ER vists across the country >10 fold!

Most related to the decorations so be careful decorating your tree! Luckily most injuries are non-fatal!
With my massive family we've seen lacerations, sprains, and most recently a pretty impressively crushed hand from a not so coordinated person carrying a heavybox, but we also had the scary moment when my 7mos old niece found her brothers toy on the ground and naturally put it in her mouth, she was fine with no ingestion or aspiration but just in case lets talk foreign body aspiration...
Normal presentations goes something like this... My child was playing on the floor and the next thing I know they were coughing and now they are making a funny noise and look like they are struggling to breath.
So what do you?
First AIRWAY of course. Does the child need immediate interventions? If so now is not the time to be a hero.. page ANESTHESIA and ENT fast! Try and maintain the child as calm as possible and in a position of comfort ( this may include keeping the kiddo head down!) Try and slip a pulse ox on and monitor but often less is more and letting the parent hold and comfort them can be better.
Get set up to intubate and have a surgical airway kit ready.
Intubating may involve pushing the object R mainstem so have all hands on deck.
For patients who are not in respiratorydistress, lets talk workup.
Starting with location.
- Laryngotracheal- uncommon but life threatening and often present in distress
- Stridor, wheezes, dyspnea, hoarse voice
- These kids need airway protection and STAT ENT and anesthesia consults!
- Try is airway protection and RIGID BRONCH

- Large bronchi-
- Cough, wheeze, hemoptysis, dyspnea, choking, SOB, decreased breath sounds
- Will also need Rigid Bronch emergently!
- Lower airway- Little distress after the initial episode
What if you're not sure and just suspect a FBA? Follow this algorithm:
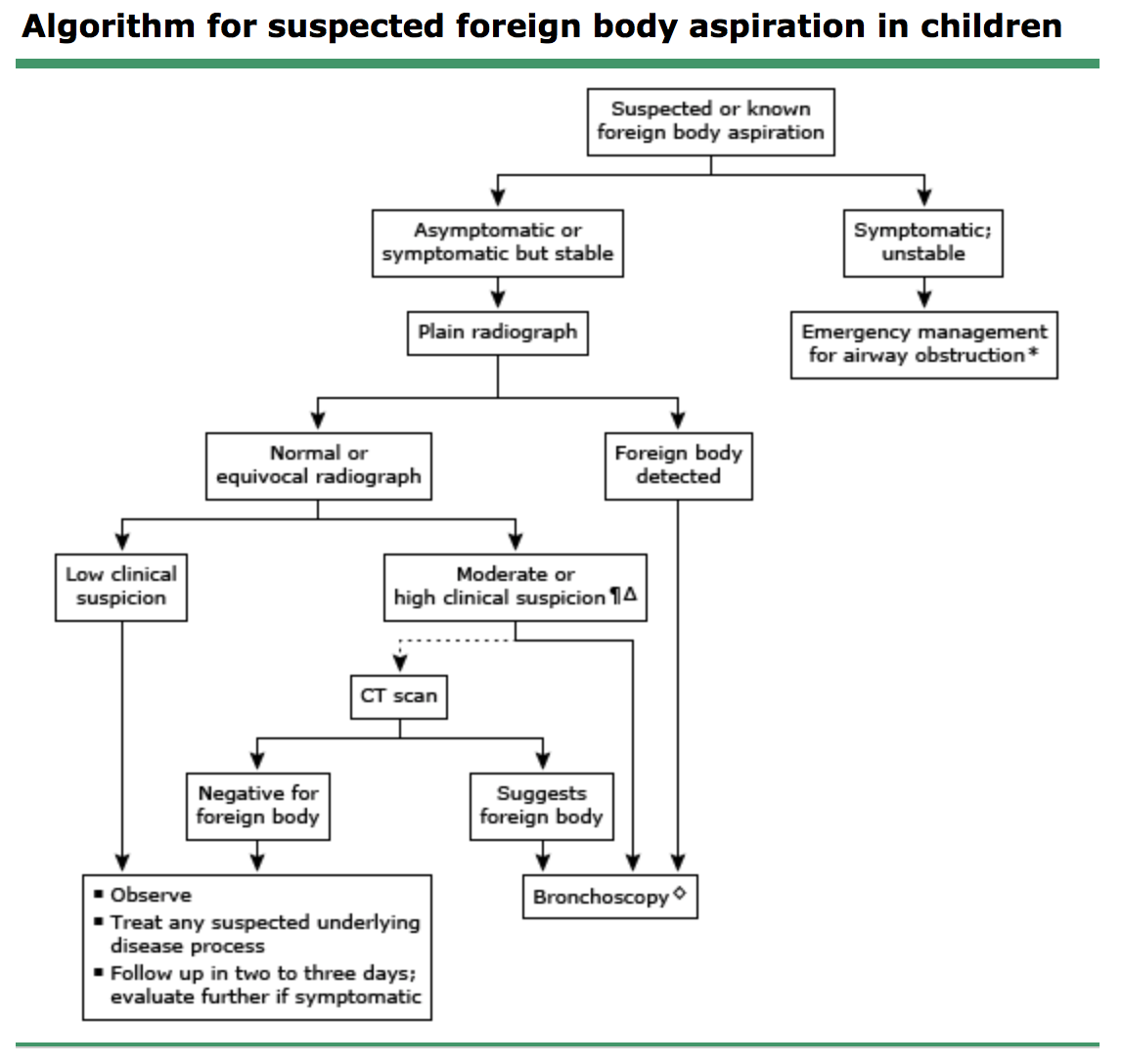
- Xrays should include inspiratory and expiratory films or Left decubitus in younger kids
- If you think its higher up inlay the neck ate PA and lateral views
- Xray findings of lower FB include:
- Hyperinflated lung- lucency distal to obstruction
- Atelectasis
- Mediastinal shift away from the FB
Management:
- All children with high suspicion of FBA should be observed and schedule for a bronch
- Rigid> Flexible as it provides better visualization and access for removal of the FB
- Thoracotomy if bronchoscopy is unsuccessful
Complications:
- Atelectasis
- Pneumonia
- Bronchiectasis
- Abx should be started post procedure
Stay safe everyone and enjoy your holidays!






