There are four degrees of carpal ligamentous injuries, each with worsening carpal instability. The most common injury mechanism is a fall onto an outstretched hand (FOOSH). Patients present with pain, swelling, and tenderness over the dorsum of the wrist. 25% of perilunate/lunate dislocations are missed on initial presentation.
Scapholunate dissociation (stage I) - Widening of the scapholunate joint by >3mm, called the "David Letterman" sign after the gap between his front teeth. This injury may require orthopedic pinning.

Perilunate dislocation (stage II) - On lateral wrist xray, the capitate will be dislocated and dorsally displaced relative to the lunate. The lunate still articulates to the radius in this dislocation.This requires emergent orthopedic consultation for reduction as this injury can be complicated by median nerve compression and avascular necrosis.

Stage III - Perilunate dislocation with dislocation of the triquetrum.

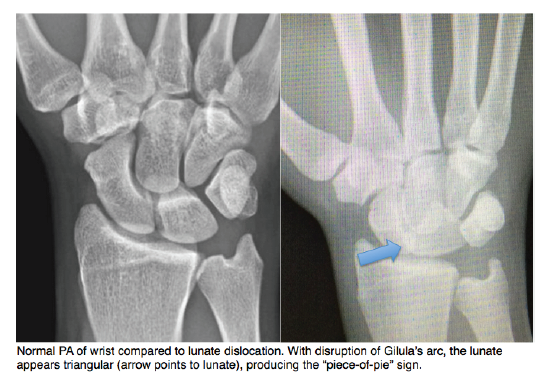
Lunate dislocation (stage IV) - The lunate disarticulates from the radius and rotates in a volar direction relative to it. On a lateral wrist x-ray you will see a "spilled teacup sign". On PA view, crowding of the carpal bones can result in a triangular-appearing lunate aka "piece-of-pie" sign. This will also require immediate reduction and splinting.
Sources
Core EM: Lunate Dislocation
Medscape: Carpal Ligament Instability
Orthobullets: Scapholunate Ligament Injury
Rosh Review