For today's POTD, we'll be taking a closer l👀k at eye pathology, specifically how we can use ocular ultrasound to further evaluate many common eye complaints encountered in the ED.
While eye complaints are fairly common in the ED, our comfort level with the diagnostic tools available to us for these complaints varies greatly.
These tools include:
- Slit lamp (the hardest part is really finding and flipping the 4 separate switches to actually turn it on)
- Fluorescein and Wood's lamp
- Tonopen (addressed in a previous POTD)
- Bedside fundoscopy (I'll admit I suck at this)
- And, ocular ultrasound!
The biggest advantage of ocular sono is how easy it is to perform.
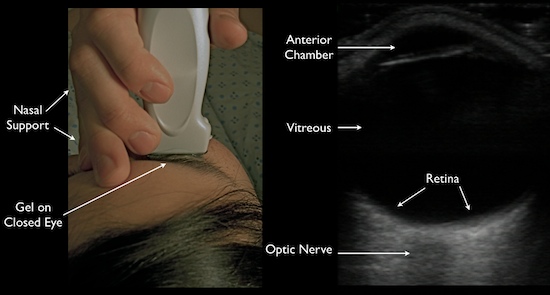
1) Slap on a tegaderm over the patient's closed eye
2) Squeeze on a generous amount of ultrasound jelly
3) Gently lay on your linear probe and look both horizontally and vertically (tell the patient to look straight ahead behind their closed eyes)
You can make so many diagnoses using ocular ultrasound!!!
- Foreign body
- Globe rupture
- Lens dislocation
- Retinal detachment
- Vitreous detachment
- Increased ICP (seen through increased optic nerve sheath diameter: measure 3 mm down, then 5 mm across)

We'll quickly focus in on retinal vs vitreous detachments. This is explained wonderfully in video form at http://5minsono.com/rdvd/, which I will summarize here.

In a retinal detachment, you can see the lines connectingto the optic nerve*. [How to remember this: the retina is just an extension of the optic nerve]
*To get a little more technical, you can also use ultrasound to tell whether a retinal detachment is "mac-on"(macula still attached, i.e. need for emergent surgical reattachment) or "mac-off" (macula detached, i.e. damage probably already done).
- The key to understanding this is knowing that the macula is located lateral to the optic nerve (or in eye-speak, on the temporal side).
- This 1 minute video illustrates the difference better than I can in words: https://www.youtube.com/watch?v=JijIfSzOG9U
- I think in reality though, if I suspect any kind of retinal detachment in a patient, whether it's mac-on or mac-off, I'll be transferring them for emergent ophtho evaluation.
 A vitreous detachment is typically seen floating above and NOT connected to the optic nerve. It is often also hazier and swirlier (very technical terms), especially as the patient looks in different directions.
A vitreous detachment is typically seen floating above and NOT connected to the optic nerve. It is often also hazier and swirlier (very technical terms), especially as the patient looks in different directions.
References:
Academic Life in EM
5MinSono.com
EMin5.com