Hypothermia is a medical emergency characterized by a core body temperature below the normal range of 95°F (35°C).
Causes of Hypothermia:
Increased heat loss
Homeless population
Elderly patients
Submersion injuries
Drugs, EtOH, CO poisoning can all cause increased vasodilation, leading to increased heat loss
Decreased heat production
Endocrine (hypothyroidism, hypoadrenalism, hypoglycemia)
Erythrodermas (psoriasis, exfoliative dermatitis, eczema, burns)
Impaired shivering
Impaired thermoregulation
Sepsis
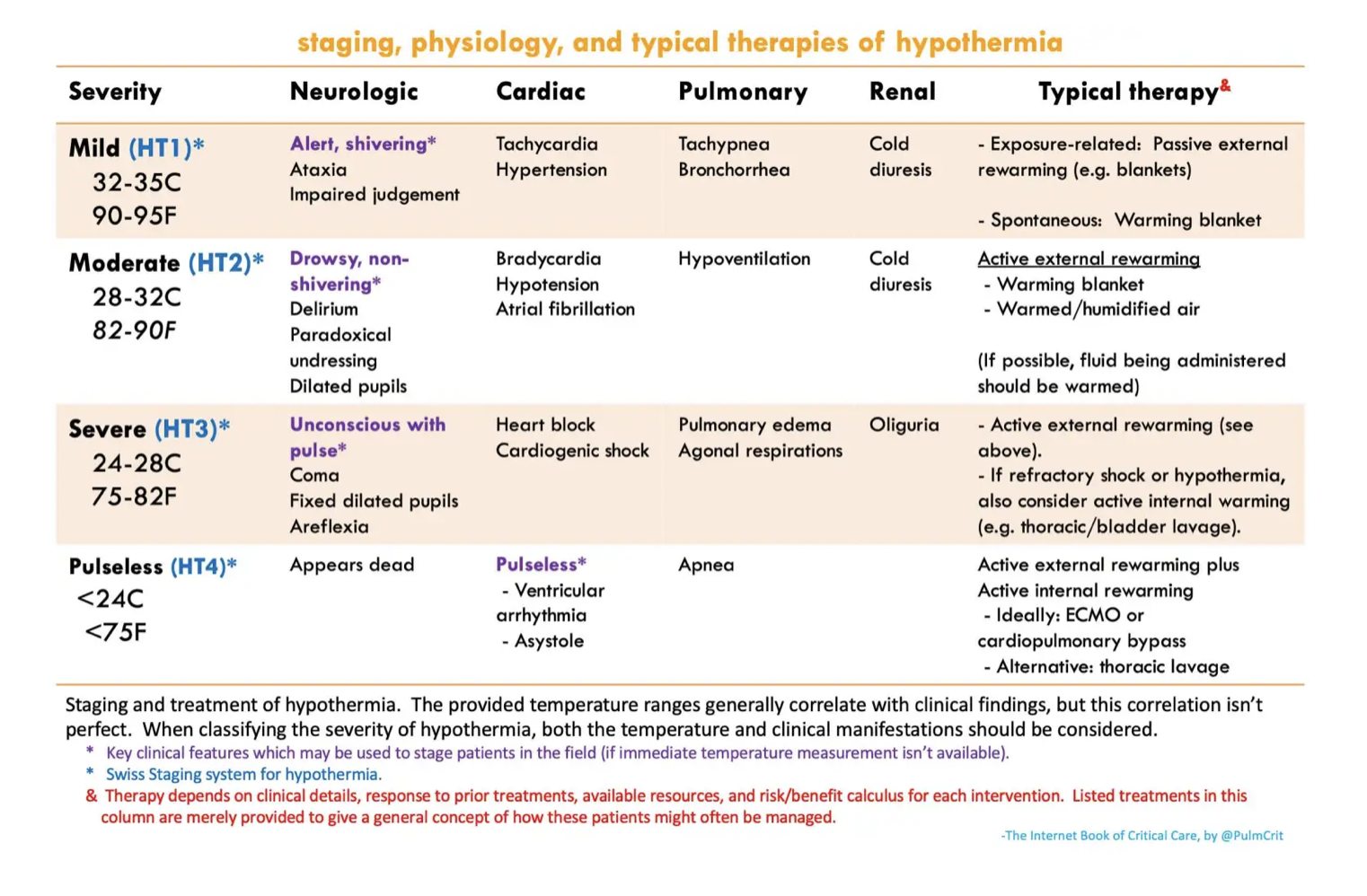
Swiss Hypothermia Staging System:
Stage 1: Mild (32-35°C) - Shivering, mild confusion, awake
Stage 2: Moderate (28-32°C) - Severe shivering, altered mental status
Stage 3: Severe (20-28°C) - Loss of consciousness, bradycardia, shivering may cease
Stage 4: Profound (<20°C) – Unobtainable vital signs
Associated Complications:
Cardiac dysfunction
Dysrhythmias can occur when body temperature drops below 30°C
There is typically a drop in temperature and MAP after rewarming is started due to vasoconstriction
Cold injuries (frostbite, etc. Maybe there will be more on this at a later date)
Coagulopathy (patient may be coagulopathic despite normal labs because the lab rewarms the sample)
Impaired clotting function
Thromboembolism (due to hemoconcentration and poor circulation)
DIC
Impaired pharmacology
Protein binding increases when temperature drops, rendering drugs ineffective
Oral meds are not absorbed well due to decreased GI motility
IM route is impaired due to vasoconstriction
Rhabdomyolysis
General Management:
Airway, Breathing, Circulation (ABCs)
Hypothermia causes a leftward shift in oxygen curve so support with oxygen, and prepare for intubation depending on how profound the hypothermia is
ECG Findings
Patients usually have sinus bradycardia, can progress to a fib with slow ventricular response
Severe cases can develop v fib
Osborn or "J" waves (associated with moderate to severe hypothermia)
Remove Wet Clothing - Prevent further heat loss
Passive External Rewarming - Insulate the patient, provide warm blankets
Active External Rewarming (should be done for moderate hypothermia)
Use forced warm air blankets or radiant heaters – our ED uses the Bair Hugger
Active Internal Rewarming (for severe hypothermia)
Warmed intravenous fluids (warmed to 38-42°C)
Heated humidified oxygen
Various lavages (Thoracic, peritoneal, bladder, GI)
Management during Cardiac Arrest:
CPR – initiate if patient does not have a pulse (should also assess if patient is still breathing)
It is challenging to assess vital signs in hypothermic patients - use end tidal or POCUS to help assist to see if patient is breathing and has cardiac function
Starting CPR if the patient does have a pulse may precipitate ventricular rhythms
Hypothermic patients have higher chances of improved neurological outcome and survival than normothermic patients that arrest
Defibrillation
Use defibrillation if indicated, but note that hypothermic patients may not respond to defibrillation until adequately warmed
ECMO
Patients with refractory hypothermia should be considered for ECMO
Patients with out-of-hospital-cardiac-arrest that are hypothermic should ideally be transported to an ECMO center
If patient is unstable (dysrhythmia, severe hypothermia, etc) ECMO teams should be contacted early in the ED visit
Stay warm out there this weekend!
Paal P, Pasquier M, Darocha T, Lechner R, Kosinski S, Wallner B, Zafren K, Brugger H. Accidental Hypothermia: 2021 Update. Int J Environ Res Public Health. 2022 Jan 3;19(1):501. doi: 10.3390/ijerph19010501. PMID: 35010760; PMCID: PMC8744717.
Baumgartner EA, Belson M, Rubin C, Patel M. Hypothermia and other cold-related morbidity emergency department visits: United States, 1995-2004. Wilderness Environ Med 2008;19:233-237
Brown et al., Accidental Hypothermia. N Engl J Med 2012; 367:1930-1938