Hello all! This week’s VOTW is brought to you by myself!
Hospital course
An 18 y/o M presented after falling off his skateboard causing him to land on his left shoulder. The XR showed a posterior shoulder dislocation, seen in the XR below where we can see the classic light bulb appearance of the humeral head.

Ultrasound
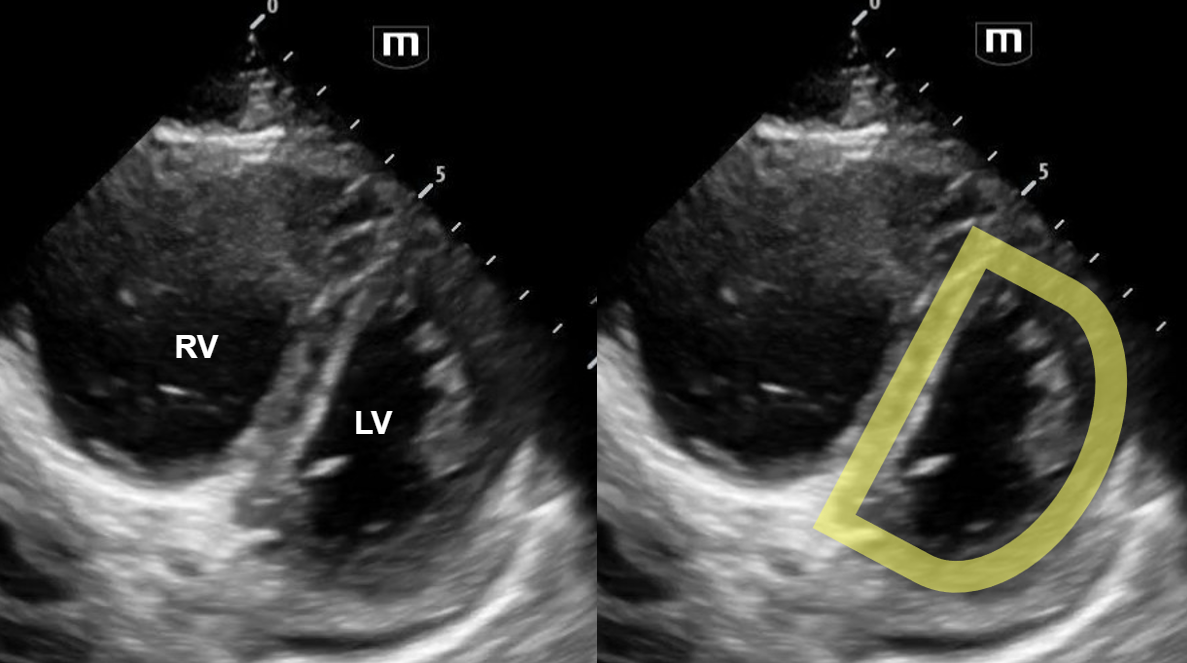
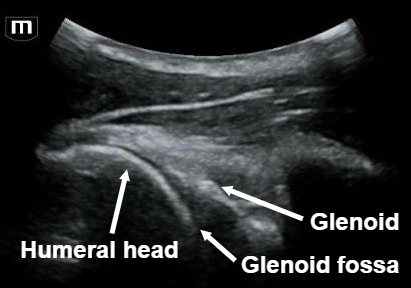
The left shoulder was scanned with ultrasound, which is shown below.
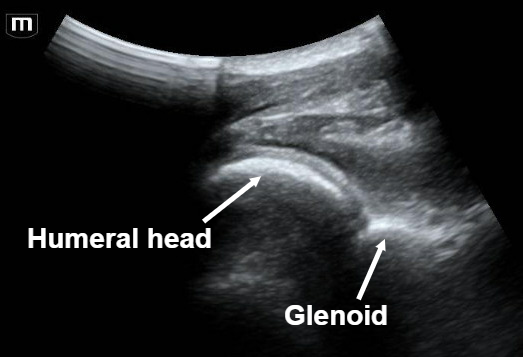
Note that close proximity of the humeral head to the probe (more superficial), which is indicative of a posterior shoulder dislocation. Also note that the glenoid fossa is not seen well, indicating that the humeral head is not articulating well with the glenoid.
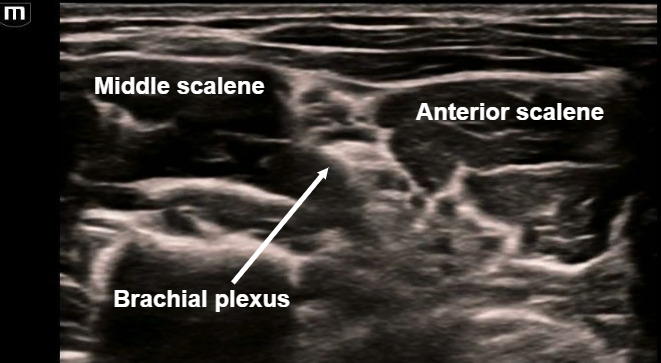
An US-guided interscalene nerve block was completed to relieve the patient’s pain. The target is the brachial plexus cords seen in the image above between the middle and anterior scalene muscles.
In the above clip, we can see the needle entering in-plane lateral to medial with injection of local anesthetic within the interscalene space, surrounding the brachial plexus.
Case Conclusion
After the interscalene block, the patient had great pain control and the shoulder was able to be reduced successfully without any procedural sedation!
This ultrasound of the shoulder was obtained post-reduction. Here we can see that the humeral head is articulating directly with the glenoid.
In this clip, we can see the glenohumeral joint with the humeral head moving well in normal alignment as the shoulder adducts and abducts.
Posterior shoulder dislocation
A posterior shoulder ultrasound scan is done by placing the probe just over the scapular spine in a transverse plane, with the probe marker towards the patient’s left.
A posterior shoulder dislocation will show the humeral head displaced closer to the probe (appears more superficial on the screen). Also, the humeral head will not be articulated with the glenoid fossa.
An US-guided interscalene block can be performed in the ED as a replacement for procedural sedation prior to shoulder reduction as seen with this patient! The interscalene block covers the shoulder and proximal humerus. The probe is placed 2-3 cm superior to the clavicle and the target is the brachial plexus which is commonly referred to as the “stoplight” sign in this view because of its 3 circular hypoechoic structures found between the middle and anterior scalene muscles.
Happy scanning!
Sono team
Resources to review: