Ever been stumped by the patient with a stubborn headache which nothing seems to be helping? An intractable migraine or relentless post-LP headache? Consider performing an SPG block.
How it works:
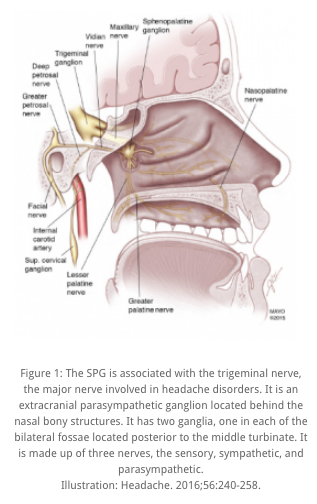
In migraines and cluster headaches, the SPG is involved in mediating parasympathetic outflow causing vasodilation of cranial vasculature. This vasodilation results in the activation of nociceptors in the meninges inflammatory mediators, resulting in classic migraine-type pain. An SPG block is theorized to mitigate headaches arising from this pathway.
How it's done:
Steps:
1. Place patient on monitor. Although you are using below-toxic dose of local anesthetic, the nasal mucosa is highly vascularized. Have patient lie supine in the sniffing position.
2. Cut off red cap from Qtip from used for swab culture; the Qtip is hollow. Using a blunt 18 gauge needle, draw up 1-2mL of bupivicaine without epithat is well below the toxic dose (ex: 2mL of 0.25% bupivicaine for 70 kg patient) into a syringe.
3. Thread the blunt needle onto the Qtip.
4. Dip the cotton end of the Qtip into 2% viscous lidocaine.
5. While patient supine and in sniffing position, GENTLY insert the Qtip straight into one nare until resistance is met. GENTLY adjust the angle slightly superiorly. Do not push against resistance.
6. Inject the bupivicaine through the Qtip.
7. Remove the syringe along with the blunt needle while keeping the Qtip in place. Instruct patient to remain supine for 10-15 minutes.
8. After 10-15 minutes, remove Qtip. If patient experiences hemifacial pain relief, offer to repeat the block via the other nare.
*note there are other variations, please see links

Note that procedure must be done with patient supine
Side effects:
Bitter taste from the anesthetic
Nausea
Local trauma causing epistaxis
Light-headedness
Numbness in the posterior pharynx
Data:
No large trials available, but small studies and case reports are promising.
Schaffer JT, Hunter BR, Ball KM, et al. Noninvasive sphenopalatine ganglion block for acute headache in the emergency department: a randomized placebo-controlled trial. Ann Emerg Med. 2015;65(5):503-510.
Jion Y, Robbins MS. The sphenopalatine ganglion (SPG) and headache. American Migraine Foundation website. Nov. 15, 2016. Accessed April 23, 2018.
Shih J, Gaafary C. Trick of the trade: sphenopalatine ganglion block for treatment of primary headaches. Academic Life in Emergency Medicine website. March 22, 2017. Accessed April 23, 2018.
Spector K, Sahai-Srivastava S. A new look at sphenopalatine ganglion blocks for chronic migraine. Practical Pain Management website. Aug, 7, 2017. Accessed April 23, 2018.
Maizels M, Scott B, Cohen W, et al. Intranasal lidocaine for treatment ofmigraine: a randomized, double-blind, controlled trial. JAMA. 1996;276(4):319-321.

