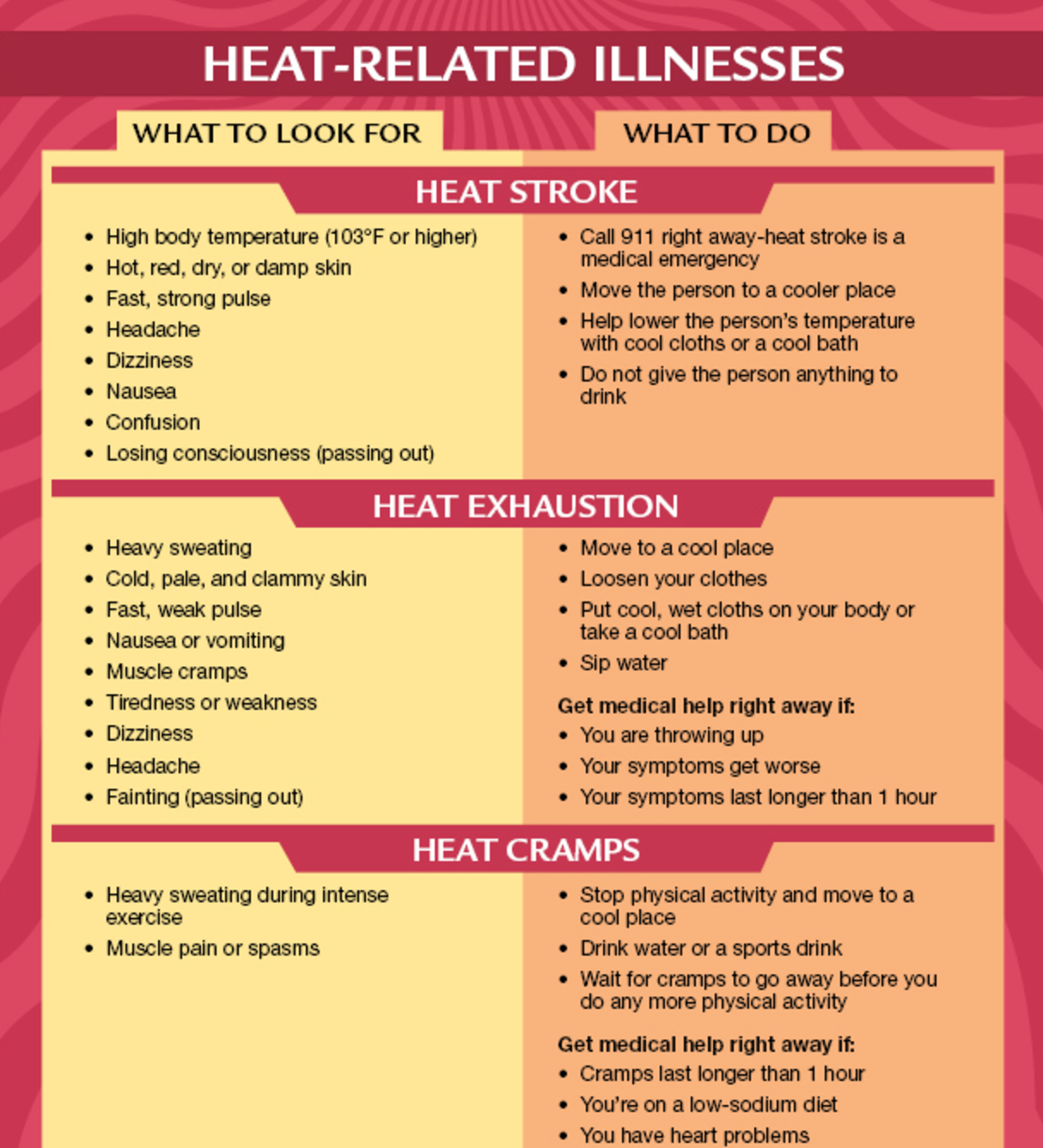
Football season is upon us and although the temperatures may feel a bit cooler, we still need to be on the watch out for HEAT STROKE. Pathophysiology:
Hyperthermia is NOT a fever which is induced by cytokine activation in response to an infection but rather an elevation in core body temperature in response to environment. We maintain our temperatures via the preoptic nucleus of the anterior hypothalamus stimulating efferent fibers of the autonomic nervous system to produce SWEATING and CUTANEOUS VASODILATION.
Evaporation is our mainstay of getting rid of heat but this becomes impaired in humid environments (75% humidity or above).
Heat stroke is considered severe if body temperature rises above 42C/108F where oxidative phosphorylation becomes uncoupled and enzymes stop working.
2 Types: Classic (nonexertional) vs Exertional
Classic-usually in the elderly, chronic medical conditions that can interfere with heat regulation (e.g. psychiatric patient on an anticholinergic like Benztropine (Cogentin) to control side effects) can cause thermodysregulation.
Exertional- usually younger, occurs during exercise in high heat/humidity such as military recruits, athletes.
Random bit of info: "Black Flag" Days in the military with >90 degree F on the Wet Bulb Globe Temperature means non-mission essential physical training and strenous exercise suspended for all personnel. 100F and 50% humidity is still under that WBGT. How many kids play sports in this weather? Yuck.
Studies to get:
CXR- you want to see if pulmonary edema has developed.
CBC, BMP for kidney function, LFTs (rarely normal if heat stroke but may not appear for 24-48 hrs. Gives us a baseline)
ABG or VBG- metabolic acidosis with respiratory alkalosis most common
PTT/PT/INR- monitor for DIC and liver damage
Urine myoglobin, CPK to monitor for rhabdo
Possibly: Head CT, LP, Tox if you think something led to them getting stuck in the sun and altered (e.g. not a clear story like a kid playing football)
Treatment:
COOL THEM DOWN! spray with water, use fans (evaporative and convective cooling!)
You can use benzos to prevent agitation and shivering (our body's way of producing heat)
Thoracic and peritoneal lavage are invasive but may be necessary. Peritoneal lavage is contraindicated in those with previous abdominal surgery or pregnant patients.
Sources:
https://www.cdc.gov/disasters/extremeheat/warning.html
http://www.med.navy.mil/sites/nhrota/explPopup.htm
