58yF with hx of CAD, DM, HTN, HLD, a-fib presents to the ED with an eye complaint - she can barely count fingers out of her left eye since this morning.
CRAO presents as abrupt and painless unilateral vision loss. It is the ophthalmic equivalent of a CVA with ischemia of the retina, and has the same risk factors. The underlying cause can be an embolus, thrombus, or vasospasm. Consider temporal arteritis in the elderly (ESR/CRP, jaw claudication, temporal tenderness). The differential for monocular painless vision loss includes occipital stroke, retinal detachment, CRVO, complex migraine.

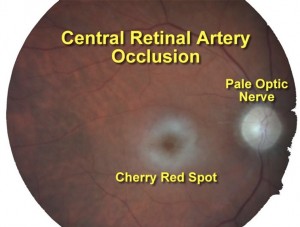
Fundoscopically, you will see a cherry red spot, vascular box-carring, and a pale optic nerve. Aside from decreased visual acuity, they may have a afferent pupillary defect on exam.
From symptom onset, there is a 90 minute window before permanent damage starts. First, call ophthalmology emergently. Then, there a number of agents and maneuvers, none of which have been proven to improve outcomes.
Dislodge embolus - Direct digital pressure through closed eyelid for 10 seconds with sudden release for 5 seconds, continue for 15 minutes
Dilate artery - Carbogen(5% CO2, 95% O2), breathing into a paper bag, nitroglycerin
Reduce IOP - topical timolol, IV acetazolamide or mannitol, anterior chamber paracentesis
However, HBOT has shown promising results and should be considered if the duration of symptoms is less than 12 hours as CRAO has a poor overall prognosis.
Sources
Rosen's
Rosh Review
emDocs: CRAO
LIFTL: Ophthamology Befuddler
Medscape: CRAO
Emergency Medicien Cases: Nontraumatic Eye Emergencies



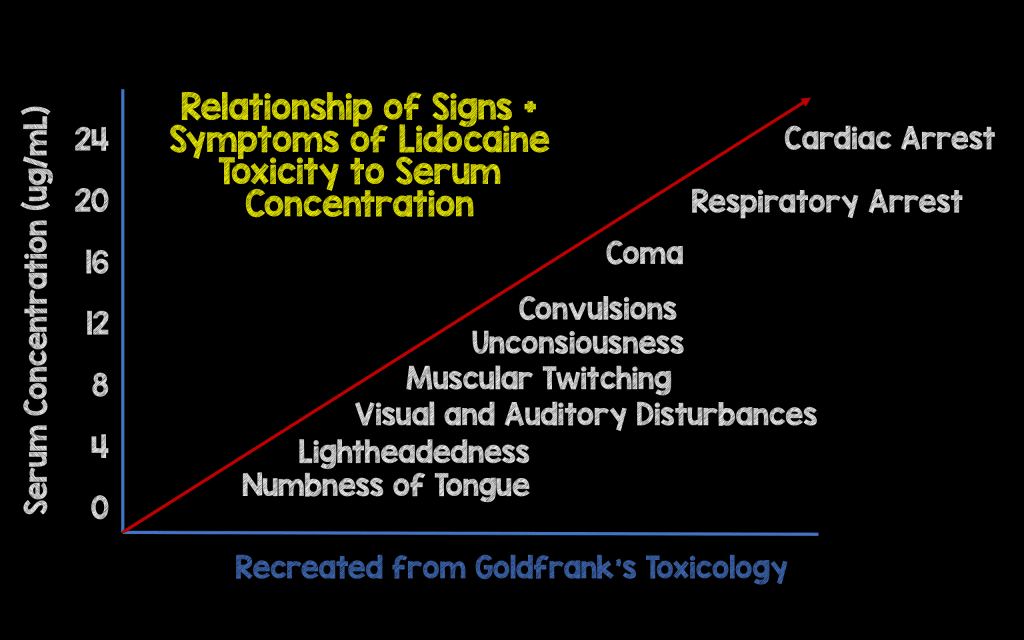
 Remember local anesthetics are sodium channel blockers, so when introduced systemically cause cardiac and neuro toxicity.
Remember local anesthetics are sodium channel blockers, so when introduced systemically cause cardiac and neuro toxicity.