Targeted Temperature Management
What is it: the purposeful cooling of a patient post-cardiac arrest. Target of 32°C to 34°C (Some studies say 36, but debatable and prevent any hyperthermia) for at least 24 hours.
Why: To improve the chance of survival and neurologic recovery, international guidelines recommend use of targeted temperature management (TTM), together with urgent coronary angiography and percutaneous coronary intervention when appropriate
Who:
Post cardiac arrest (any cause but most evidence supports from VF/VT shockable causes of cardiac arrest)
ROSC < 30 mins from team arrival
Time < 6 hours from ROSC
Patient is comatose, GCS <8 (this is try and improve neurological outcome, so someone who is neurologically intact does NOT need TTM)
MAP >= 65mmHg
depends on your hospital protocol
When: Initiate within 6 hours of ROSC and maintain for 24 hours
How:
cold IVF at 2-3 mL/kg stat
cooling vest and cooling machine
sedation and paralysis

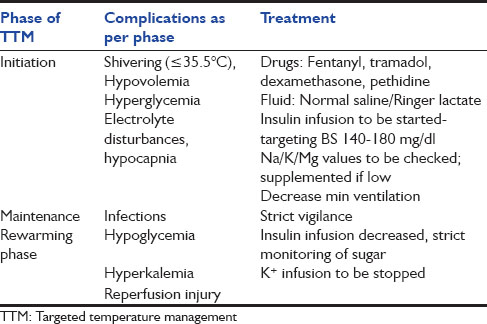
Complications:
Shivering, electrolyte abnormalities, cold diuresis, infection.
So, for post cardiac arrest patients with depressed neurological function - Keep this in mind, but consult your ICUs and plan this patient's care together for best management. TTM needs an ICU level care admission.
Happy Learning!
References:
https://jamanetwork.com/journals/jama/fullarticle/2645105
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4578199/
https://lifeinthefastlane.com/ccc/therapeutic-hypothermia-after-cardiac-arrest/
http://www.ijccm.org/article.asp?issn=0972-5229;year=2015;volume=19;issue=9;spage=537;epage=546;aulast=Saigal